The last HbA1c I had before starting on the pump was 5.8 % (Nov. 14 2005). In April this year, when I started pumping, the aim of my diabetes nurse and I was to try to increase this just a little (to 6.0 %) to see if this would also eliminate some of the nasty lows that had experienced. While these nasty lows were not that numerous after the switch to Lantus 3 years ago, they would occasionally show their ugly face, usually leading to a trip to the ER or a visit from the paramedics in our home, so I sure would like to get rid of those.
As described in previous posts, the switch to the pump still has to prove its worth in relation to lows. Because of that I wasn't too surprised to see a slight decrease in my HbA1c at my endo appointment in the end of June, almost 3 month after pump start. At that time it was 5.7 %, which would be great if it wasn't because of all the lows it included.
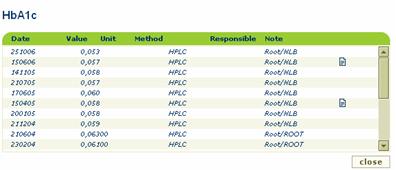
Last week I mailed another sample for HbA1c-analysis. Sunday evening I went into my web health portal to see if the result was back yet. It was. I have an appointment with my diabetes nurse this Thursday, and I am looking forward to see her reaction to the result. 5.3 % it said, which is the lowest it has been since I moved to Odense in the beginning of 2001.
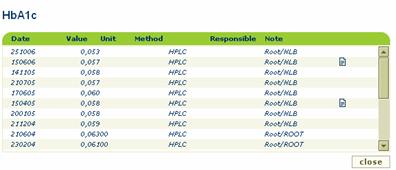 My HbA1c results the past 2 years
My HbA1c results the past 2 years
Before that I had results as low as 5.1 %, which at that time was more a concern to my doctors than to me, because I didn't had that many low, and certainly not as many requiring assistance in their treatments as I have had afterwards, even with higher A1c's.
 My HbA1c results the past 2 years
My HbA1c results the past 2 yearsBefore that I had results as low as 5.1 %, which at that time was more a concern to my doctors than to me, because I didn't had that many low, and certainly not as many requiring assistance in their treatments as I have had afterwards, even with higher A1c's.
I will have to admit that the perfectionist inside me most certainly aims for an A1c that is normal, i.e. in non-diabetic range (4.6-6.4 % as far as I remember from patophysiology classes). Not at any costs though. The current 5.3 % result, while in this range, stores too many low lows. I cannot remember ever having tested, or even being able to test, at 1.1 (20) or lower (my meter just reads LO for values of 1.1 and below) in all the years I was on MDI. I have already lost count on the number of times this has happened while on the pump, but it is at least a handful of times. Of course these lows are somehow outweighed by the highs that has also been present, especially after soccer games, but that just shows that the BG-curve has not leveled out as much as anticipated. Hopefully this will happen with time, but it is a bit difficult to be patient, when you were promised results, potentially within 3 months.
It may sound like I am all negative about the pump and the promises that comes with it. That is not the case. I certainly see advantages with this therapy as well. I am probably just, still, a bit frustrated by the fact that I cannot seem to get a hold of things with CSII, and that it regularly causes issues that are not only troublesome but also scaring at times. I hope that my next A1c will be as great as this one, only without the hypoglycemic backside of the result :-)



{kind=link}