Hope you all had a joyful Christmas! Mine was okay.
The evening before Christmas, we spend with Jimmi’s mother and her boyfriend, a very relaxed evening - despite the intensity of the rolling-dices-for-presents-game (everyone brings some small presents specifically to this game. You role a dice, and every time you get a 6, you are entitled to pick a present on the table. When all presents have been picked, a timer is set and the game continues, only now, when you get a 6, you pick a present from one of the other players).
Christmas morning Jimmi and I went to the local zoo, as entry was free between 10:00 AM and noon. When leaving, we talked to one of the inspectors at the entry, and she said that in these two hours more than 5,200 people had entered the zoo. The weather was nice, so it was actually a great opportunity, especially to families with younger children, to get out and use a bit of time and energy walking around the park.
We spend Christmas eve at Jimmi’s father’s house with his wife, Jimmi’s younger brother, S (11 years old), and their sweet little dog, Fido. We had a three-course dinner (split into two, because S was too excited about lighting the Christmas tree and getting presents). Appetizer: Rice porridge with cinnamon. Main course: Duck and roast pork with potatoes, potatoes in caramel coat (they are called “brunkartofler” in Danish, and are essentially small potatoes that are coated with a mixture of warm, liquid sugar and butter in a frying pan until they are warm and coated with this brown sugary stuff. Yum!!), red cabbage, prunes, and apples and jelly – a typical Danish Christmas dinner. Due to the excitement of S, we then danced around the Christmas three – Fido joined us, not really knowing what this was all about, but she definitely did not want to be left out of it, much to our joy – singing a few song and then S was allowed to distribute presents. When everybody had opened their presents, we went back to the table for dessert: Ris a la mande (the dictionary says it should be called rice pudding, although I don’t think that is quite the same) with cherry sauce. There was a bit discussion about who actually got the whole almond hidden in the dessert, and therefore, who was entitled to the almond-price, but as the dispute was between S and his father the price stayed in the family :-)
Christmas day (Dec. 25) my parents stopped by as they had taken my sister back to see her new apartment. Otherwise the day was used to relax.
The second Christmas day (Dec. 26) was used on Christmas lunch – again at Jimmi’s father’s house – allowing us to also say hello to Jimmi’s younger sister and her boyfriend. They live in
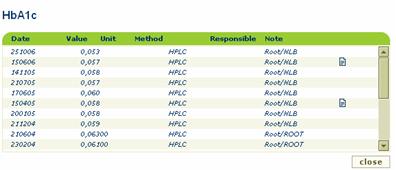
My BG-levels behaved very well during the Christmas days. Almost all readings was in range, only a few outliers – 2.0 (36) being the lowest and 9.8 (176) being the highest. I have been experimenting a little with the use of the dual wave bolus for more meals, and it does actually seem to smooth sugars out even more.
Overall this would make a very nice Christmas if it wasn’t for the early “Christmas present” that I got just 4 days before Christmas, and people, of course, couldn’t help asking about – explanation follows!
December 20 was the big clean-up-and-Christmas-lunch-day at work. Everyone had been assigned to an area, in order to keep everyone busy and make sure that every inch of the lab and mass spec-rooms would be cleaned. It worked very well. After a common breakfast in the coffee-room – to make sure that everyone had energy to use for the clean-up ;-) – we swirled through the labs leaving them clean as ever. I worked with a couple of post-docs in the back part of the main lab. We worked pretty effectively, so by 11:30 AM we were done, and since the lunch was not until 1:00 PM, we took a round to make sure no one else needed help before we drifted back to our offices to clean up there.
I share my office with 3 master students, none of them being there for the clean-up. One of them was excused, though – she went into labor that day, and by the end of the day she had given birth to a beautiful baby girl :-) Being the only one in my office, I could of course be tough and throw out everything that didn’t have a name on it, but I refrained from doing that and just focused on my own stuff (which, by the way, takes up most space in our small office). When I could actually see my desk again, I checked my mail. I was excited to see a mail regarding the PhD-application I just managed to send in before deadline end of November. I knew that the assessment committee was to meet at December 18, and I was told that they expected to be able to give answers to the applicants before end of December. To receive a mail regarding the application less than 2 days after the assessment committee meeting, what could that mean? Was it rejected or accepted?
I opened the mail, and was referred to an attachment. I opened the attachment and couldn’t help scanning it quickly – only to find out that I had not been chosen to receive a stipend :-( I then carefully read the letter. They had found my application to the specific project very qualified (no kidding – the project was about mass spectrometric quantitative phosphoproteomics in mitochondria from T2 diabetic muscles, and I have worked with quantitative proteomics in my Master’s and am currently working with phosphoprotein analyses, having 6 years of mass spectrometry experience plus a lot of knowledge about diabetes!), but they had found another candidate to be better qualified! My initial thought – besides disappointment – was “Who the hell could that be?”
I ranted a bit about this rejection to a couple of people, including Jimmi of course, and decided that I would question my supervisor, who happens to be one of the supervisors on that project too, about what qualifications I was missing. Just before the lunch I ran into him in the hallway, asking him: “So, I heard that someone but me was better qualified for the project….?”
“Yeah, I had the chance to place both Z and you in Ph.D-positions, and we (as in you and I) have this meeting with W from Hamburg in January, so Z was given this one – but I would like to discuss this with you”, he replied.
“Sure” I said, while inside me anger was starting to build – in close contact with the aforementioned disappointment!
I didn’t enjoy the lunch as much as I had wished to, and really just wanted to go home early. Before going home however, I wanted to discuss the issues with my supervisor, since I wasn’t sure when he would leave for the Holidays (turned out that this was actually his last day and he wouldn’t be back until beginning of January). Fortunately, he had the time to talk that afternoon.
“I didn’t know that you had applied for that stipend” he said, closing the door to his office.
I told him that I saw the advertisement just 3 days before deadline, and he was out of the house at that time so I didn’t have the possibility to discuss it with him, but as he had mentioned it to me earlier in the fall, before it was announced, and because the deal with this guy from Hamburg is far from settled yet, I saw no reason not to apply for this.
He could understand that. He then told me that he had encouraged Z – one of his Master’s student, who just graduated the week before - to apply for this stipend, and that we were both very qualified for this project, but he thought that it might be good for me to get away from our lab for a while – once again mentioning the up-coming meeting with W from
I told him that I of course do not intend to never leave the university, but that I was beginning to loose patience a bit, and therefore saw nothing wrong in applying for whatever possible positions and project of my interest.
I guess this actually requires a bit more background for you to understand my reaction. You see, when I graduated in October 2005, I clearly stated to my supervisors that I would like to obtain a PhD-position, in case they came across something. Back in the beginning of summer my supervisor at the university was contacted by this guy, W, in
My supervisor and I agreed that we would have to get clear-cut answers from W regarding his search for other working places, as well as the exact project plans before agreeing to anything. I believe I got my point about impatience through, as my supervisor continued to say that if we could agree to start the project, then he wouldn’t mind aiming for a start in March, or whenever it would fit W, relieving me from my current contract, which otherwise does not terminate until May. So far so good. Still, I just have a feeling that I need to be prepared for something else, if this Hamburg-deal doesn’t work out. Therefore I am currently signing up for the competition about other PhD stipends other places too, so that I will have something to fall back on, just in case.
In hope of a Happy New Year fellow bloggers!













{kind=link}